Conferences and Capital The 2026 Workforce Shift
27 Jul, 2026


Never has a pharma or biotech’s use of capital been under more scrutiny. Consequently, regar...

Never has a pharma or biotech’s use of capital been under more scrutiny. Consequently, regardless of size, the goal posts and calculus required to place good bets on the right assets that demonstrate the greatest likelihood of clinical and commercial success have moved significantly. And while these decisions have increased in complexity, the hand-over and inherent risk in clinical and commercial execution to outsourced providers remains unchanged.
With over 75% of program budgets going to clinical development, outsourcing service providers have become a mainstay of the industry; positioning themselves as willing and able to assume clinical activities viewed traditionally as “non-core” to the sponsoring company. And more often than not, this had made sense, especially when considering the related costs and infrastructure needed for sponsors to conduct clinical trials themselves. Unfortunately, service levels and performance of these externalized relationships haven’t been consistent and frequently result in an innovator being forced to choose the best, worst option – where the larger clinical research outsourcing (CRO) providers lack the flexibility to accommodate (and prioritize) smaller programs while the smaller providers, although more nimble, may not have the complete toolkit and experiences required. This has become more acute post-pandemic, post-“COVID bump”, over the past 18-24 months.
The Contract Research Outsourcing (CRO) industry experienced a notable deceleration in 2024. This slowdown, while indicative of broader economic and market trends, also presents a unique opportunity to re-evaluate the existing sponsor-CRO relationship and provide an alternative to a decades-old model built on the backs of blockbuster therapeutics.
The slowdown may be attributed to a confluence of factors: general post-pandemic demand correction, slower VC investment in biotech and emerging pharma R&D, the Inflation Reduction Act's provisions for Medicare drug price negotiation and inflation-based rebates forcing portfolio reshuffling/re-valuation, as well as the non-reauthorization of Priority Review Voucher (PRV) programs used to incentivize the development of new treatments in less prevalent yet critically underserved populations. The latter introducing a significant challenge for future pharma and VC investment alike.
All of this underscores the need for a more agile and collaborative approach to clinical research and how sponsors manage their clinical development programs. Traditionally, Full-Service Providers (FSPs) and Contract Research Organizations (CROs) have been the go-to solution, offering perceived advantages in scale, expertise, and global reach. However, for many sponsors, a compelling case can be made for bringing clinical trial management back in-house. This white paper explores the strategic merits of a new in-house approach; powering a means to retain control of high-value programs, while providing the required strategic and operational expertise to enhance efficiency, reduce costs, and ultimately accelerate the delivery of life-changing therapies to patients.
Revisiting the definition of “In-House”
The traditional CRO model is commoditized, highly competitive and often a taxing choice for sponsors; delivering a rigid and transactional experience to sponsors (especially on the smaller end) who seek a more ‘white glove’, nuanced experience. Biotech and emerging pharma are often looking for a 3-D printed solution versus the standard high-overhead, bundled service approach provided by a traditional CRO. FSP is seen as more of an opportunity in the space, however, outsourcing entire functions for long periods of time locks-up capital that may otherwise be reallocated during lulls in functional need.
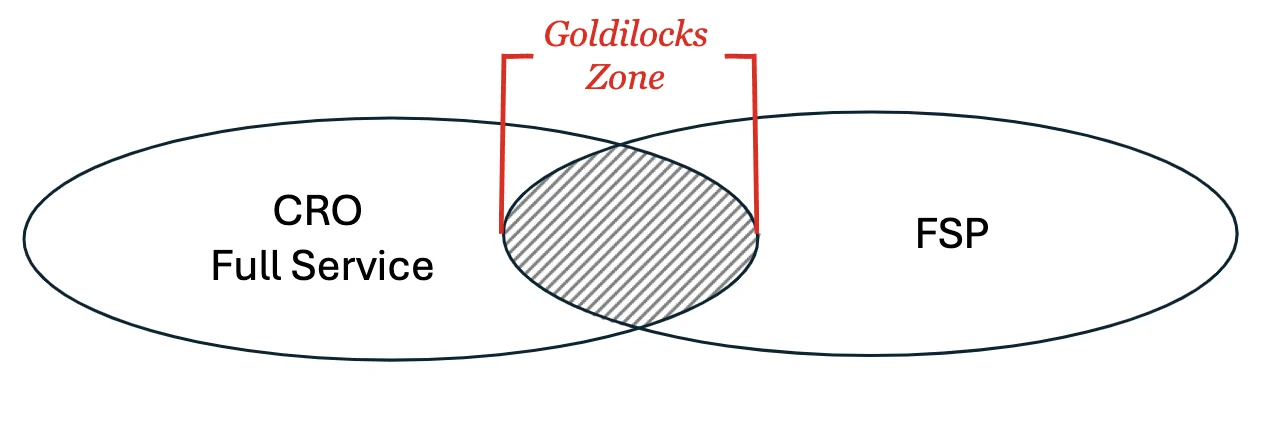
There is an opportunity for innovators somewhere in the middle – to define a space that is in the Goldilocks zone; being overall quite familiar and easy to navigate, but with a couple of powerful strategic differences built in.
To clarify the distinction, we can consider five fundamental models for conducting clinical trials, each with varying degrees of internal and external involvement, and assesses them across several dimensions critical to drug development. These models range from "Fully Internal," where all aspects of the trial are managed by the sponsor, to "Full-Service Outsourcing (FSO)," where external partners handle most or all functions. In between are a spectrum of hybrid approaches that vary in control, cost and responsibility. Key operational aspects such as talent, technology ownership, adherence to SOPs, and data integration are used to differentiate these models.
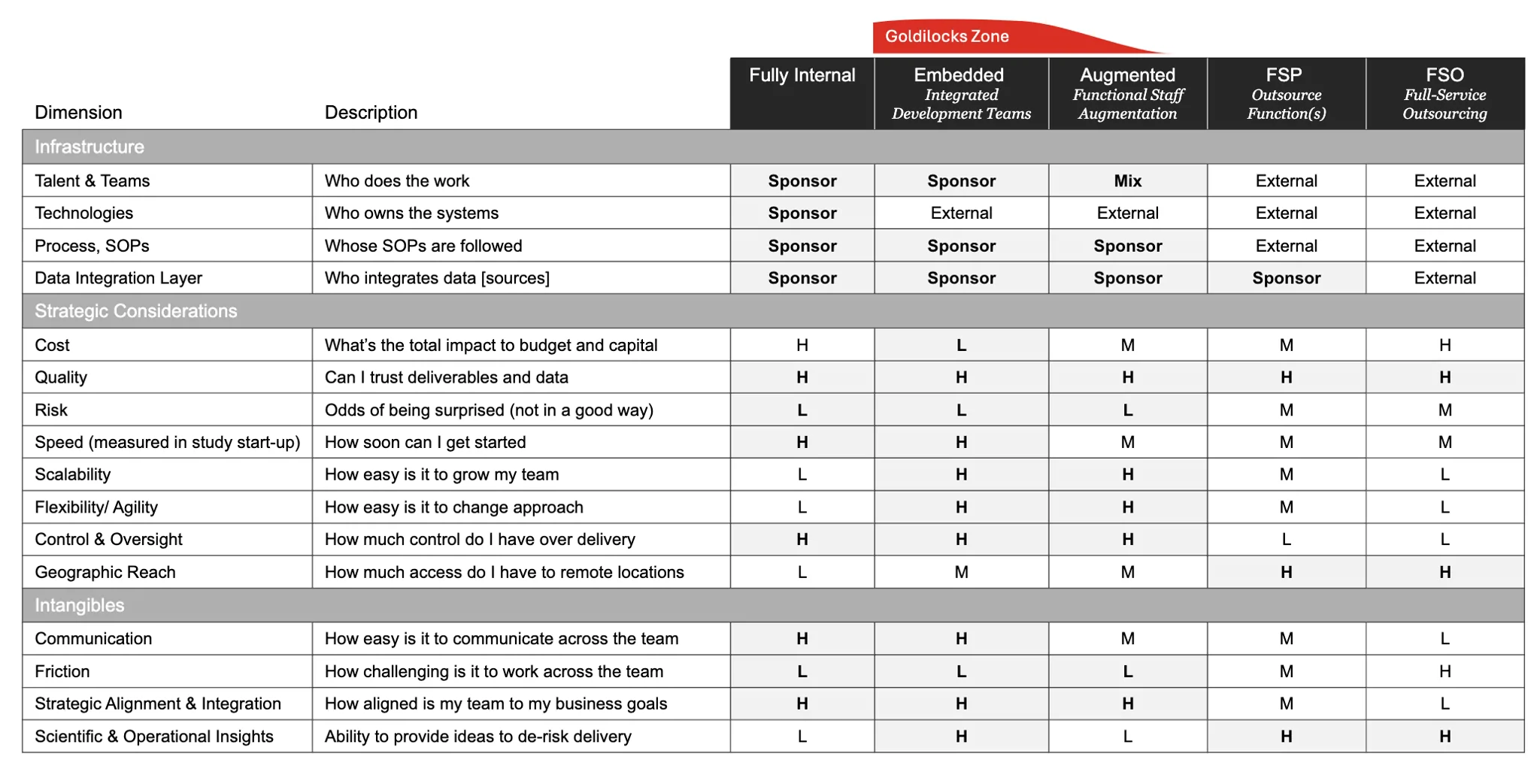
To be clear, the way to think about in-house isn’t to stand-up a full clinical development and operations organization internally, but to leverage strategic sourcing in a new way – a way that embeds integrated development teams into your organization. This new model, for the purposes of this paper we are calling “Embedded”, provides teams of contingent SMEs and operators that can fully execute your program end-to-end.
Critically, Embedded Development Groups/Teams (EDG), can be plugged in at any point within your program’s lifecycle. EDG teams can be built based on your design and readily integrated into your organization; allowing you to keep operational delivery close, and your core team lean while affording your business maximum optionality and agility as your program needs change over time.
How it works
Similar to a traditional CRO model, four roles in the EDG model work closely with a sponsor to facilitate the clinical program: a general program partner or executive lead, an operations lead, a resourcing lead, and a project lead.
General partners are product developers and asset strategists with over 20 years in (s)mid-to-large pharma and biotech and are responsible for the overall assembly, conduct and quality delivery of integrated embedded teams.
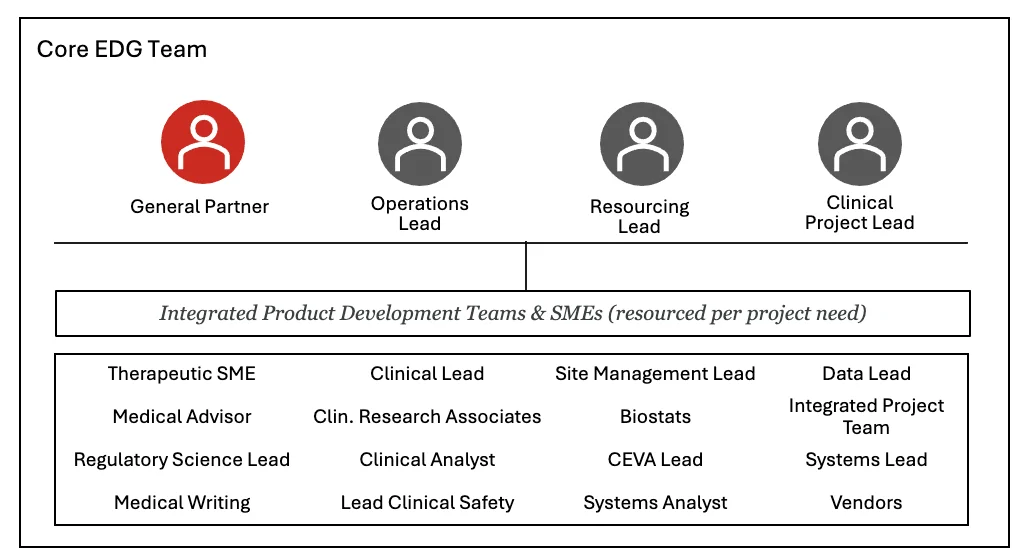
The EDG core team has access to a curated network of SMEs and “A-team” operators who would be dedicated to your program until the end.
Core responsibilities are divided across the team and evolve throughout your program.
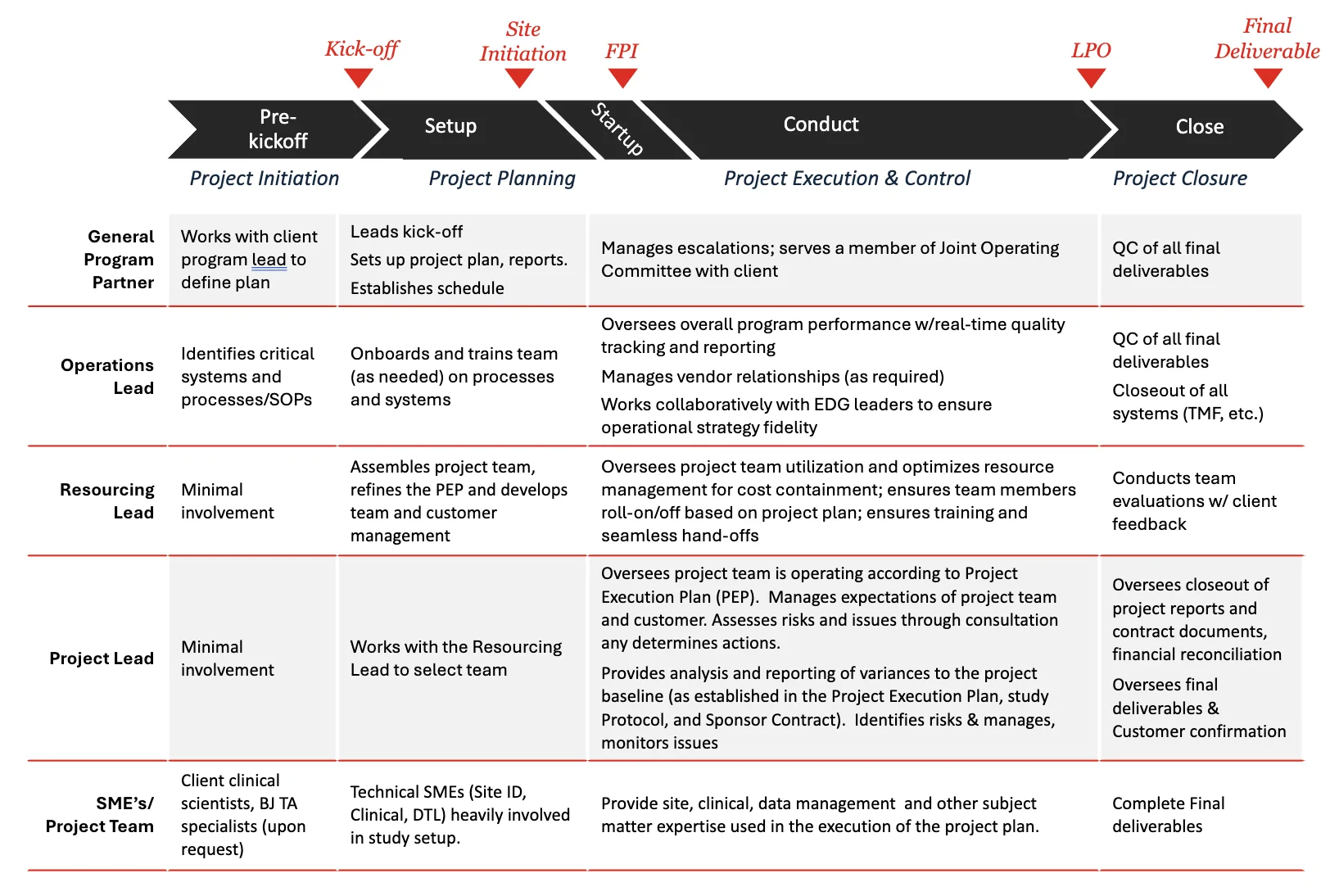
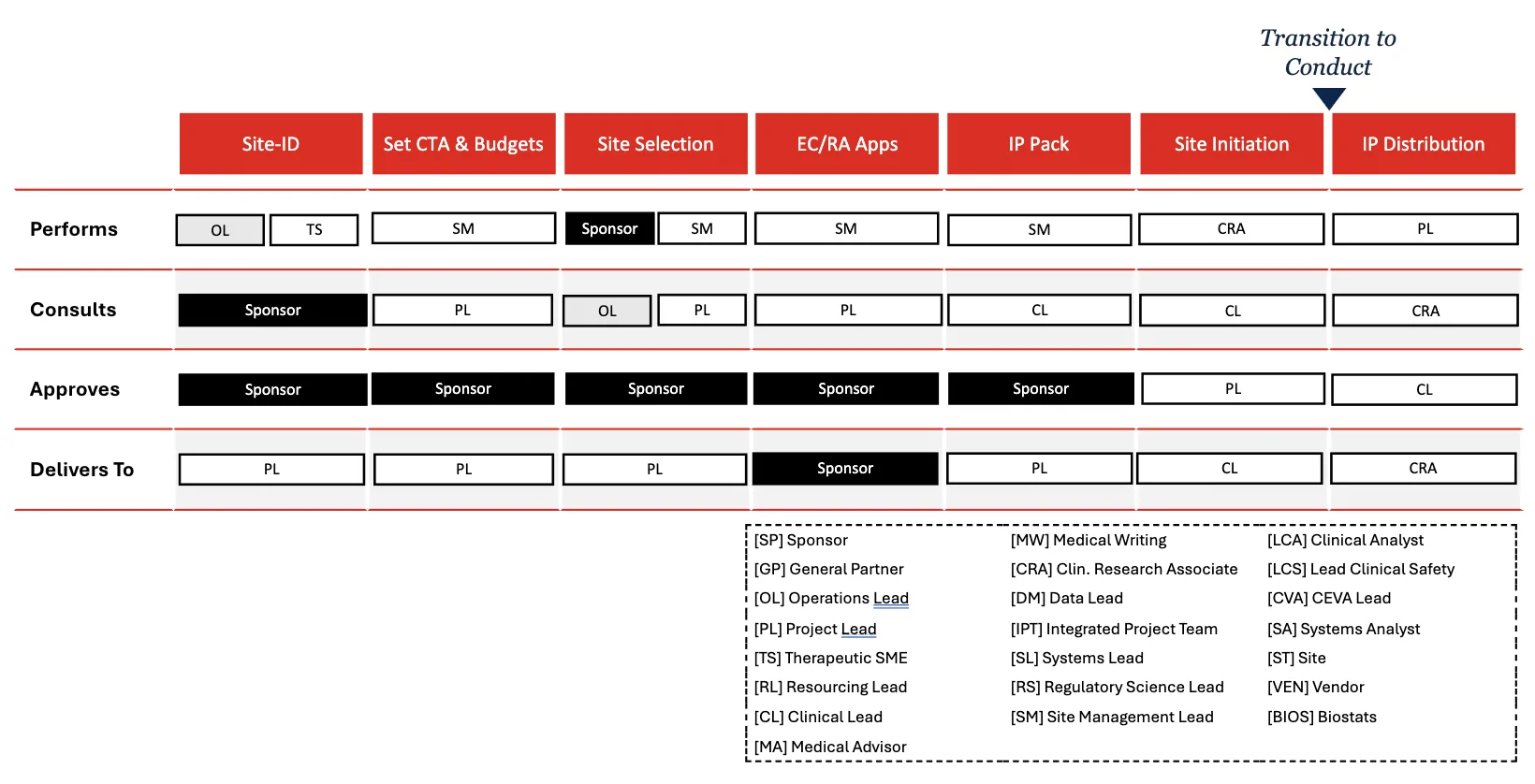
However, where and how these roles participate may vary significantly depending on the degree of participation and role the sponsor wishes to play. For example, if we double-click on the ‘setup’ and ‘start-up’ stages of a clinical program, a white-boarding discussion with the sponsor may result in the following example division of responsibilities:
Set-up
Key Deliverable(s):
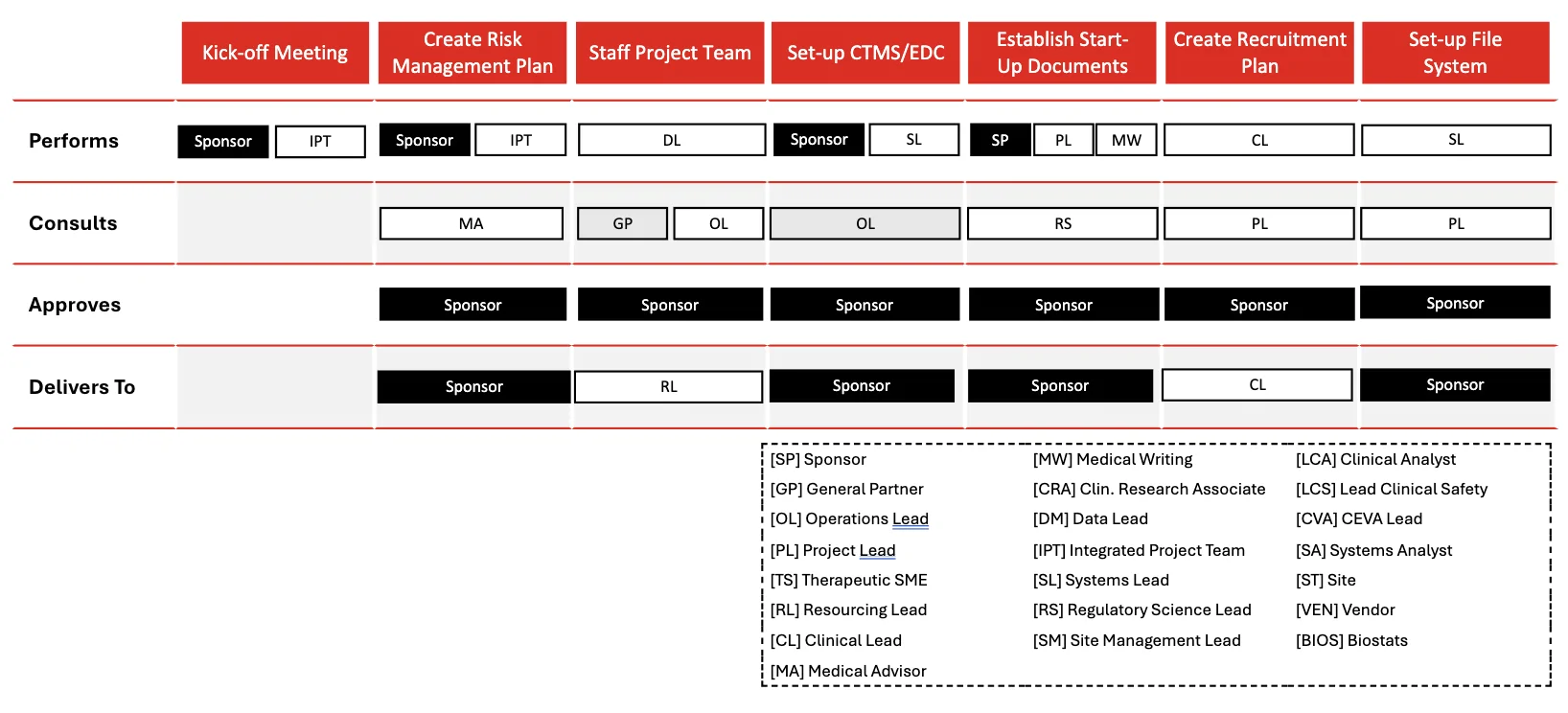
Note that those roles and responsibilities not run by the sponsor or indicated as those run by the general partner, the operations lead, or resourcing lead, would be contingent resources brought into the company to execute the associated activities.
Start-Up
Key Deliverable(s):
EDG Benefits
The overarching goal for any biotech company is to efficiently and effectively bring safe and efficacious therapies to market, ultimately improving patient lives and delivering value to stakeholders. Achieving this requires rigorous clinical development that is not only scientifically sound but also strategically aligned with the company’s core mission and long-term vision. In this context, the decision to manage clinical trials in-house rather than relying on external providers like FSPs or CROs emerges as a powerful strategic alternative. This approach directly addresses several critical objectives that are often diluted or less optimally achieved through traditional outsourcing:
Enhanced Control and Oversight
One of the most compelling arguments for the EDG clinical model is the unparalleled level of control and oversight it affords. When a biotech company manages its trials internally, every aspect of the process – from protocol development and site selection to data collection, monitoring, and regulatory submissions – remains under direct corporate purview. This direct command extends to expedient decision making, integrated quality assurance (rather than an outsourced function) and greater operational visibility.
Deep Therapeutic Area Expertise and Institutional Knowledge
Your programs are inherently specialized, focusing on specific therapeutic areas or modalities. The EDG model allows for the cultivation and retention of deep, proprietary expertise in these niche areas that benefits future development programs.
Additionally, uncommon cross-functional synergies across the business that ensures that clinical strategy is deeply informed by scientific discovery and that clinical findings rapidly feed back into early-stage research, become realized; accelerating the development cycle and optimizing pipeline decisions.
Agility and Responsiveness to Dynamic Environments
The clinical trial landscape is constantly evolving, influenced by scientific breakthroughs, changing regulatory requirements, and competitive pressures. EDG teams are inherently more agile and responsive to these shifts.
Immediate Cost Efficiencies and Value Retention
EDG teams can be set-up rapidly (by CRO standards) and eliminate the standard overhead and markups and help you realize immediate savings over the course of one clinical program, let alone a portfolio. Resources are ring-fenced and optimized for the specific activity – which contrasts with traditional CRO engagements characterized by ‘A’ team swaps for ‘C’ team players.
Conclusion: Embracing the Embedded Model for a Resilient Future in Clinical Development
The landscape of clinical development is undergoing a profound transformation. As highlighted throughout this paper, the traditional reliance on external Contract Research Organizations (CROs), while historically prevalent, is increasingly proving to be a suboptimal strategy for many pharmaceutical companies, particularly in the wake of recent market decelerations and evolving industry dynamics. The "best, worst option" dilemma, necessitates a fundamental shift in how clinical trials are managed and executed.
The Embedded Development Group (EDG) model emerges not merely as an alternative, but as a superior strategic imperative for both biotech and pharma companies. By strategically embedding contingent SMEs and operational teams directly within the sponsor's organization, the EDG model offers an unparalleled level of control and oversight, ensuring that every aspect of the trial remains under direct corporate purview. This integrated approach fosters expedient decision-making, enhances quality assurance, provides greater operational visibility and most importantly – no surprises. Perhaps most compelling are the immediate cost efficiencies and value retention that the EDG model delivers.
Ultimately, the goal for any pharmaceutical or biotech company is to efficiently and effectively bring safe and efficacious therapies to market, improving patient lives and delivering value to stakeholders. The decision to manage clinical trials through an Embedded, in-house approach is a powerful strategic move that directly addresses these critical objectives. It is about reclaiming control, fostering innovation, and building a resilient, agile, and cost-effective clinical development capability that is truly aligned with the company's core mission and long-term vision. Embracing the Embedded model is not just about overcoming current challenges; it's about future-proofing R&D and accelerating the delivery of life-changing therapies to patients.
Get in Touch
To explore how Barrington James Strategic Solutions Group can become a trusted partner in your organization’s long-term success, connect directly with our leadership.
Contact:

Bryan Katz
President, Barrington James Strategic Solutions Group
BKatz@barringtonjames.com

Stowe Milhous
Client Services Director, Barrington James Strategic Solutions Group
SMilhous@barringtonjames.com

