The Rise and Growth of Antibody-Drug Conjugates in Cancer Treatment.
18 Jun, 20253 minsAntibody-drug conjugates have arisen as a groundbreaking class of targeted cancer therapies,...
Antibody-drug conjugates have arisen as a groundbreaking class of targeted cancer therapies, often described as "biological missiles" due to their ability to deliver potent cytotoxic drugs to tumor cells. The newsletter this week researches the ascent of ADCs from the first FDA approval in 2000 to the latest developments in 2025, covering history progression of ADC approvals, R&D pipeline highlights, market growth trends & forecasts and development challenges.
Historical Progression of ADCs
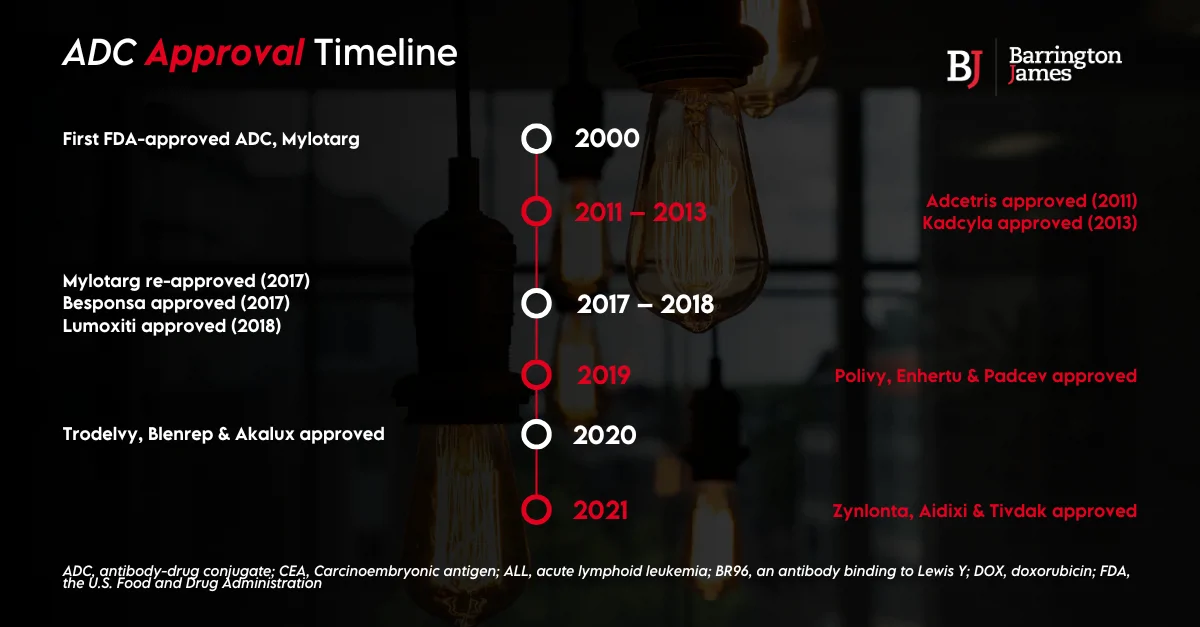
The ADC era began in 2000, when the FDA granted approval to Mylotarg (gemtuzumab ozogamicin) for acute myeloid leukemia (AML), making it the very first ADC on the market. Mylotarg couples an -CD33 antibody with a calicheamicin toxic and demonstrated the concept of targeted delivery of chemotherapy. The rollout however, suffered challenges such as severe toxicities which led to Mylotargs withdrawal in 2010. Importantly, during the 11 years following the debut of Mylotarg, no new ADCs reached the market. It was only after dose optimization and further studies into Mylotarg, which earned re-approval in 2017 for a sample size of AML patients, highlighting the learning curve in developing safe and effective ADC dosing regimens.
Momentum returned in 2011, when Adcetris targeting CD30- positive lymphomas, validated modern linker and payload chemistry. Following on from this, we saw Kadcyla, the first solid tumour ADC for HER2- positive breast cancer. From 2017 onwards, approvals accelerated with Besponsa in 2017, Lumoxiti in 2018, and a trio in 2019 including Polivy, Padcev, and Enhertu expanding into both hematologic and solid tumours. Between 2020 to 2022, we saw Trodelvy in 2020, then Zynlonta and Tivdak in 2021, and Elahere in 2022. This wave pushed the FDA roster to roughly to 13 distinct oncology ADCs by late 2024. The total is continuing to rise, datopotamab deruxtecan secured approval in early 2025 and telisotuzumab vedotin won accelerated approval in May 2025, bringing the count toward 15 and confirming that ADCs have evolved into a broadly validated therapeutic class.
R&D Pipelines and Promising Candidates
Advancements in linker chemistry, payload diversity, and anti-body engineering have bloated the APC pipeline from “more than 100 clinical candidates” recorded in late 2021 to 200+ molecules in trials and 500+ in pre-clinical work as of 2025. A 2024 landscape audit of 168 active assets show that that ≈85% now target solid tumours importantly breast and lung cancer marking a decisive shift away from the haematology-heavy first decade of ADC work. This range spans across 60+ antigens and a growing mix of site-specific conjugations, novel linkers, and non-traditional payload classes which has further emphasized the global R&D investment in the modality.
Three late stage programmes are building out the next wave. Datopotamab deruxtecan (Dato-DXd), a TROP-2-directed ADC from Daiichi Sankyo/AstraZeneca, secured FDA Priority Review in January 2025 on the back of positive TROPION-Lung data and could become the first TROP-2 ADC for EGFR-mutated NSCLC. Merck and Daiichi Sankyo have co-developed Patritumab deruxtecan (HER3-DXd) which is showing to be clinically meaningful in PFS in HER3- expressing EGFR-mutant lung cancer, even after resistance to TKIs, although its BLA initially faced withdrawal pending overall survival confirmation, signalling continued refinement rather than failure.
Late-stage highlights
- Datopotamab deruxtecan (Dato-DXd) – Trop-2-directed; FDA Priority Review for EGFR-mutated NSCLC.
- Patritumab deruxtecan (HER3-DXd) – HER3-directed; clinically meaningful PFS in resistant EGFR-mutant lung cancer.
- Telisotuzumab vedotin – c-MET-directed; accelerated FDA approval in 2025 for high-MET NSCLC.
Market Growth, Investment Trends, and Forecasts
Pfizer's $43 billion takeover of Seagen on 2023 started off an M&A surge that has established as a strategic pillar for Big Pharma. Soon after, Merck pledged up to $22 billion to co-develop three Daiichi Sankyo DXd conjugates, including patritumab deruxtecan, in one of the most lucrative licensing deals on record.
This buying frenzy carried on into 2024 with Abbvie acquiring ImmunoGen for over $10 billion to secure Elahere and its IGN platform, Johnson & Johnson paid $2 billion for Ambrx to access next-generation conjugation technology, and AstraZeneca followed its earlier $6 billion upfront alliance with Daiichi Sankyo by committing $1.5 billion to build a fully dedicated ADC plant in Singapore, reinforcing long-term manufacturing confidence.
These capital infusions are translating into robust market growth. IQVIA data shows ADCs accounted for about $18 billion in global cancer drug spending in 2024 with double-digit expansion projected through 2029. Market researches broadly agree on the trajectory, with Research & Markets sizing the sector at $7.8 billion in 2024, rising to $11 billion by 2030, while MarketsandMarkets and Grand View expect $19–24 billion over the same horizon, and contract-manufacturing analyses forecast revenues topping $25 billion as capacity builds out and new indications launch. These monumental M&A transactions represent the growth ADCs from niche innovation to a core oncology revenue machine, with investors and manufactures positioning for sustained and high-growth returns.
Development Challenges
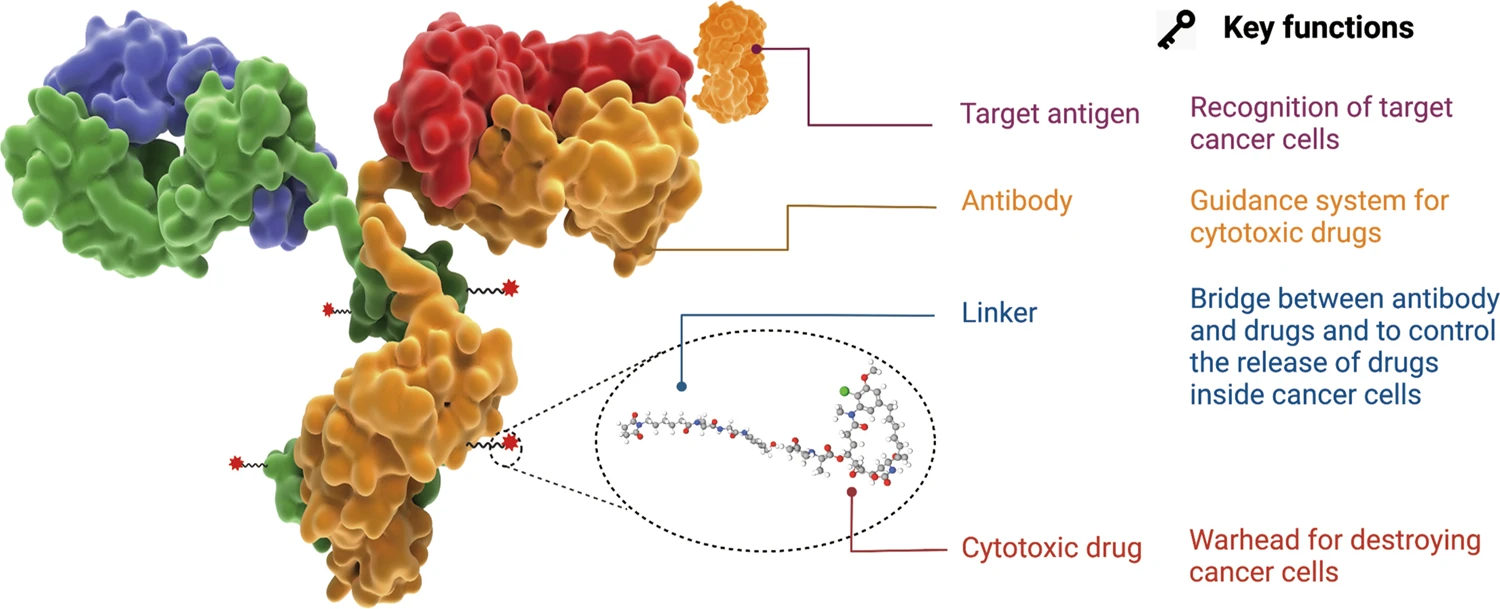
Building an effective ADC means balancing antibody, linker and payload to deliver cytotoxin to tumours while sparing normal tissue. First generation agents such as Mylotarg relied on acid-labile hydrazone linkers that leaked calichamicin in plasma, driving off-target toxicity and prompting the drugs withdrawal in 2010.
Second and third generation designs adopted cleavable linkers and increasingly site specific conjugation, which yielded more homogeneous drug-to-antibody ratio and sharper tumour selectivity. Some products carry particular risk, Blenrep was pulled from the US market in 2022 after corneal toxicity could not be reduced, while HER2- directed Enhertu and Kadclya included boxed warnings for potentially fatal interstitial lung disease.
Beyond safety, developers must be able to navigate pharmacokinetics including linker stability, DAR, and target-mediated uptake creating multiple circulating species whose exposure is incredibly difficult to model. The complex and expensive process of conjugating high-potency toxins to biologics in commercial manufacturing creates an additional barrier, necessitating the investment in specialised CDMOs and plants.
Why Partner With Barrington James
If you are ready to bring your project from idea to market, partnering with Barrington James allows you to tap into a global network of specialized talent built up over more than 23 years. Our specialized consultants work within niche sectors and can work side-by-side with your leadership to establish high-performing teams through the entire development cycle.
Whether you’re seeking specalized talent, exploring career opportunities, or looking to stay informed with the latest industry insights, our team is dedicated to connecting you with the resources you need. Discover how our specialized expertise in Life Science staffing can drive your growth and innovation.
Visit our website to secure the talent that will drive your success and subscribe to our newsletter for exclusive industry insights, market trends, and expert perspectives in life sciences staffing.
Related Posts

Celebrating Clinal Trials Day 2026
20 May, 2026